Article Text

Statistics from Altmetric.com
Introduction
Capillary refill time (CRT) is defined as the time taken for colour to return to an external capillary bed after pressure is applied to cause blanching.1 It was first described in 19472 and has since become widely adopted as part of the rapid structured circulatory assessment of ill children. Its use has been incorporated into advanced paediatric life-support guidelines, and it is endorsed by many national and international groups. However, despite its ubiquity there is a great deal of variation in how CRT is performed, and little knowledge of factors which may affect its accuracy. In this article, we will give an overview of the use of CRT in children and how its results should be interpreted.
Physiological background
CRT is dependent on the visual inspection of blood returning to the distal capillaries after they have been emptied by the application of external pressure.1 The physiological principles which underpin peripheral perfusion are complex and affected by many different factors.
Capillary blood flow is affected by the driving pressure, arteriolar tone and the constituents of the blood. The driving pressure is influenced by hydrostatic pressure (blood pressure) and, at the level of capillaries, oncotic pressure due to plasma proteins.3 Arteriolar tone depends on a delicate balance between vasoconstrictive (noradrenaline, angiotensin II, vasopressin, endothelin I and thromboxane A) and vasodilatory influences (prostacyclin, nitric oxide and products of local metabolism such as adenosine). The constituents of blood can also impact on capillary blood flow. For example, the size of red blood cells and plasma viscosity can affect flow through narrow capillaries.4 The other main determinant of capillary perfusion is capillary patency which is reflected by the functional capillary density or the number of capillaries in a given area which are filled with flowing red blood cells.1
Vasoconstriction is considered an early compensatory mechanism to shock which should reduce distal capillary bed perfusion. It is hypothesised that alterations in capillary bed perfusion will affect the measurement of CRT by altering the time for the external capillaries to become refilled with blood. A prolonged CRT should, therefore, act as an early indicator of shock.1 It has also been investigated as a marker of response to treatment, such as fluid boluses or inotropes.5
Technological background
The first use of CRT was described in World War 2 to estimate the degree of shock in battlefield survivors.2 At this time the categories used were imprecise, consisting of ‘normal’, ‘definite slowing’ and ‘very sluggish’, which corresponded to ‘no’, ‘slight’/’moderate’ and ‘severe’ shock, respectively. In 1981, Champion proposed incorporating CRT as one of the five elements of a trauma score.6 An upper limit of 2 s for CRT was arbitrarily chosen as normal and has since become widely adopted across the published literature.
Perhaps surprisingly, there is no clear consensus on exactly how CRT should be performed in children. Table 1 details some of the methods which have been described in the published literature. In general, it is recommended that pressure is applied, usually to a distal finger or nail bed or the sternum, for a variable time of between 3 and 5 s to cause blanching. The time taken for colour to return after the pressure is removed is then measured. Figure 1 demonstrates the technique for performing CRT using the index finger in a child. Figure 2 shows CRT being performed on the sternum in a neonate.
Different methods of measuring CRT in children

A demonstration of the technique for capillary refill time in the index finger of a 1-year-old. (A) Pressure is applied to the distal nail bed for 3–5 s to cause blanching. (B) The time taken for colour to return is measured.
{kind=link}
{kind=link}
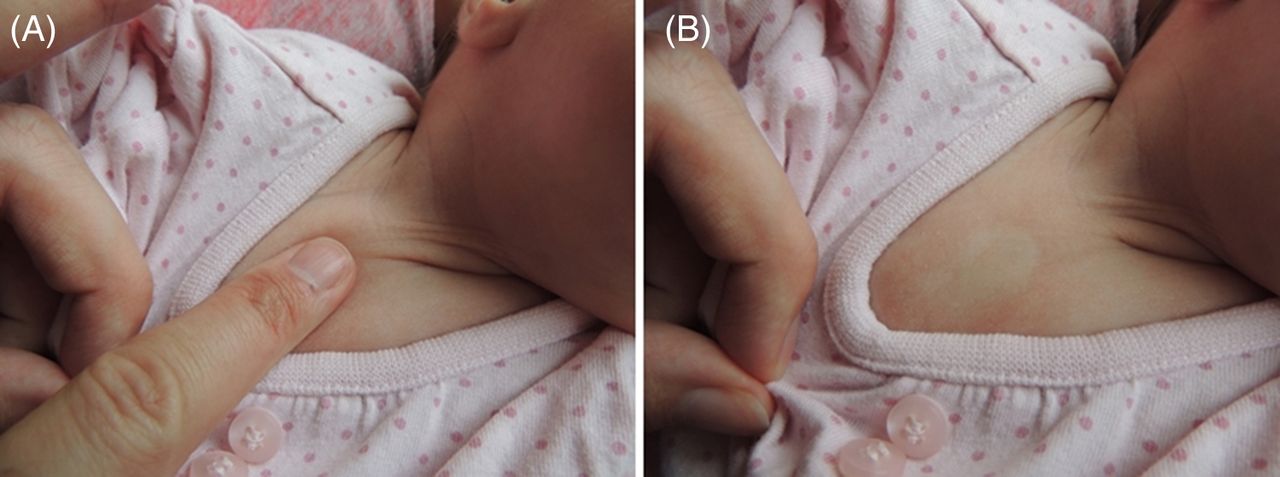
A demonstration of the technique for capillary refill time on the sternum in a neonate. (A) Pressure is applied to the sternum for 3–5 s to cause blanching. (B) The time taken for colour to return is measured.
Although several different sites in the body can be used to check CRT, there is no convincing evidence that one is more accurate than another. In normal neonates, CRT has been shown to be longer if it is measured at the heel compared with the head or sternum.7 In this population, CRT should, therefore, probably be checked at the sternum or forehead in preference to a peripheral digit. However, the only study to compare CRT at different body sites in normal children concluded that fingertip CRT was significantly faster than CRT measured at the sternum.8 In view of this uncertainty, perhaps what is most important is to ensure that the site at which CRT is checked is clearly documented and that the same site is used during assessment and after any treatment.8
Various studies have been performed in an attempt to determine what the length of CRT should be in normal children. Schriger and Baraff examined 100 healthy children aged between 2 weeks and 12 years and found that 95% have a CRT less than 1.9 s.9 Saavedra et al10 also reported that the upper limit of normal for CRT was 1.5 s in 30 well children aged 2–24 months. However, a more recent study, which examined 92 healthy children aged 0–12 years found a significant minority of normal children had a CRT between 2 and 3 s, with the longest having a CRT of 2.78 s.8
Studies examining CRT in neonates are much clearer, that a normal CRT can be slower than 2 s in this age group. Raju et al11 examined 137 healthy newborn infants between 1 and 120 h of age, and showed that the mean CRT was 4–5 s in the hands and feet with some babies having a CRT of up to 9 s. However, some of these infants were examined immediately after birth when birth-related events may have had an impact. Strozik et al7 also examined CRT in 469 normal neonates and stated that the upper limit of normal was 3 s.
In summary, the literature shows that a normal CRT can probably be between 2 and 3 s in children, and as long as 3 s in neonates.
Indications and limitations
The clinical situations in which CRT can be useful are discussed below. When assessing CRT, healthcare professionals should also consider the external factors which may affect its accuracy. These are detailed in box 1.
External factors which may affect the accuracy of capillary refill time (CRT) in children and neonates.
Temperature: Gorelick et al21 measured the CRT of 32 healthy children who had been assigned to either a warm (mean temperature 25.7°C) or cool environment (mean temperature 19.4°C) for 15 min. Children who had been in the cool environment had a significantly prolonged CRT compared with those in the warm environment. Only 31% in the cool environment had a CRT <2 s, whereas, those in the warm environment all had a CRT of <2 s. It is debatable whether fever has an effect on CRT. CRT has been shown to decrease in adults as core temperature increases.22 However, the only study in children showed that patient temperature had no effect on CRT.23
Ambient light: A study in 309 adult participants compared the measurement of CRT in daylight conditions to the measurement of CRT in dark conditions. In dark conditions, CRT was unable to be accurately assessed in 66.7% of the subjects compared with 3.9% in daylight conditions.24
Site of measurement: CRT has been shown to be longer if it is measured at the heel than the head or sternum in neonates.7 Paradoxically, the only study which has examined the effect of site on CRT in older children concluded that fingertip CRT was significantly faster than CRT measured at the sternum.8
Pressure application: There is no clear consensus on exactly how long pressure should be applied to measure CRT, with most guidelines stating between 3 and 5 s. However, in neonates, it has been shown that applying pressure for a prolonged time (3–4 s) compared with a brief time (1–2 s), can significantly increase CRT.25
Interobserver reliability: Initial rapid partial refilling of the capillaries may be followed by a slower complete filling, and defining when this has finished is subjective. In general, the literature suggests that there is not good agreement when different observers measure CRT. In a study of 46 nurses and nursing assistants who were shown a video of adults having CRT measured, there was only moderate agreement for the exact value of CRT and what constituted normal.26 Otieno et al also showed that there was not good agreement between four different observers when measuring CRT in 100 children admitted consecutively to a hospital in Kenya. However, agreement between observers did improve when the CRT was short (<1 s) or long (>4 s).27
In children at risk of dehydration, does a prolonged CRT help to identify children who are dehydrated?
The majority of the literature indicates that CRT is useful in the assessment of children with dehydration. Steiner et al systematically reviewed the use of CRT to detect dehydration greater than 5% in children. They included four studies in their analysis and a total of 478 participants. Although they remarked that all the included studies had a variety of methodological weaknesses, they concluded that a CRT >2 s predicted dehydration in children with a sensitivity of 60% and a specificity of 85%.12 There is, therefore, reasonable evidence that CRT may be useful in assessing children at risk of dehydration.
In children and neonates, does a prolonged CRT correlate with other important physiological measurements of perfusion or cardiac output?
There are several studies which have attempted to validate the use of CRT by assessing its correlation with other physiological measurements of systemic perfusion or cardiac output. These have had mixed findings. Raimer et al5 found that a CRT in children of ≤2 s was predictive of superior vena cava (SVC) oxygenation saturations of ≥70% with a sensitivity and specificity of 84.4% and 71.4%, respectively. Goal-directed resuscitation in septic shock targets superior vena cava (SVC) oxygen saturations ≥70% as one of its therapeutic endpoints, as this has been associated with superior outcomes. Appraising their findings, Raimer et al concluded that a CRT of ≤2 s may be a useful therapeutic endpoint for goal-directed therapy in the treatment of septic shock.
CRT has also been investigated in preterm neonates by comparing it to SVC flow as determined by echocardiography. Low SVC flow has previously been validated as an accurate reflection of systemic blood flow in neonates, and has been shown to be associated with low urine output, mortality and poor neurodevelopmental outcome.13 Central CRT was compared with SVC flow in 128 preterm neonates which showed that a CRT of ≥3 s had a sensitivity of 55% and a specificity of 80% for predicting low SVC flow. The authors suggest that although CRT alone is an imperfect measure of SVC flow, the two are certainly correlated. They also showed that combining a CRT of ≥3 s with a low mean blood pressure (BP <30 mm Hg) provided a better prediction of low SVC flow with a sensitivity of 78% and specificity of 63%.13
However, other studies have not shown that CRT correlates with important physiological parameters. CRT was compared with cardiac output in 58 children undergoing cardiac catheterisation. There was no significant correlation found between the CRT taken at the time of cardiac output measurement and measured cardiac output.14 Another study examined a group of 55 children admitted to ICU with either cardiac or non-cardiac (mostly septic) illnesses. This study compared a CRT of <2 s with various haemodynamic variables including cardiac index, central venous pressure, systemic vascular resistance index, stroke volume index and blood lactate. In cardiac patients, CRT was not found to correlate with any of these variables, while in non-cardiac patients it only weakly correlated with stroke volume index and blood lactate. The authors concluded that a CRT of <2 s had little predictive value and was not useful in the population of patients they had studied.15
In neonates with suspected sepsis, does a prolonged CRT increase the risk of proven bacterial infection?
In a recent study of 170 predominantly preterm neonates (average gestation at birth of 28 weeks) with signs and symptoms suggestive of sepsis, a prolonged CRT was shown to be a strong independent marker for late-onset bacterial infection.16 Late-onset bacterial infection was defined as a proven infection occurring after at least 4 days of life. A prolonged CRT (defined in this study as >2 s), which was measured over the sternum, was seen in 50% of neonates with late-onset bacterial infection, compared with only 10% without. A prolonged CRT, therefore, gave a sensitivity of 50% and a specificity of 90% for proven bacterial infection in the population studied. If prolonged CRT was combined with one or more raised inflammatory markers, the sensitivity for detecting bacterial infection increased towards 100% although there was a corresponding reduction in specificity. It is interesting that the authors of this study chose the threshold for an abnormal CRT as >2 s when the majority of the literature indicates up to 3 s in neonates is probably normal. Nevertheless, this study does support the clinical utility of CRT in assessing neonates with suspected sepsis.
In children presenting to primary or secondary care, does a prolonged CRT at initial assessment increase the risk of serious illness?
The other main area in which CRT has been studied is as a predictor of illness severity. There is increasing evidence that children with a variety of different illnesses have worse outcomes if they have a prolonged CRT at initial assessment. Seven hundred children who presented to a large paediatric assessment unit in England had a number of vital signs recorded, including CRT. Children who had a serious infection, such as pneumonia, meningitis or a bacteraemia, were significantly more likely to have a CRT>2 s compared with children with mild infections.17 However, it was only a minority of children who had a prolonged CRT with most children with a serious infection having normal perfusion. A large systematic review of clinical features which may be useful in predicting serious illness in children also confirmed that a prolonged CRT is one of the strongest indicators of serious illness in children.18 The authors again highlighted the poor sensitivity of this finding with it only being present in 10% of children with serious infections.
The value of CRT in identifying children at risk of serious illness has also been proved in less developed nations. In a prospective study of 2446 children with severe and complicated malaria in Ghana, a CRT>2 s at presentation more than doubled the risk of death. Again, although highly specific, a prolonged CRT was not very sensitive in predicting mortality, with most children who died having a normal CRT when they were initially assessed.19
In summary, it would appear that a child is much more likely to have a serious illness if they have a prolonged CRT, and that this is true across a variety of healthcare settings. Importantly though, a normal CRT does not mean that the child does not have a serious illness.
Topics for further research
A number of different methods of measuring CRT automatically have been described. These hope to eliminate the effects of interobserver variability and inconsistent pressure application. One potential approach uses digital videography which replaces visual observation by substituting an electronic image sensor for the human eye. This is known as digitally measured CRT (DCRT). In 83 children assessed as having mild dehydration by clinicians, DCRT was found to more accurately predict the presence of significant dehydration (>5%) compared with clinical assessment.20 Another method of automated CRT assessment uses a photoplethysmographic sensor based on a blue-light emitter, although formal trials of its usefulness are awaited.1
It is possible, that methods which use automated CRT may become more widespread if they are demonstrated to be helpful in the assessment of unwell children. However, only a small number of trials have so far assessed their effectiveness and further research is required.
Clinical bottom line
-
CRT is performed by applying pressure to an external capillary bed to cause blanching and measuring the time taken for colour to return.
-
Normal children can have a CRT between 2 and 3 s, and normal neonates can have a CRT up to 3 s.
-
CRT is useful in the assessment of children at risk of dehydration, and a prolonged CRT increases the risk of serious illness in unwell children; it may also be useful in identifying infection in neonates.
-
CRT can be affected by ambient temperature, ambient light, the site of measurement, the amount of pressure applied to the capillary bed, and is also subject to interobserver variability.
-
CRT should always be judged within the clinical context, and is rarely useful in isolation.
Test your knowledge
-
How long can CRT be in normal neonates?
-
1 second
-
2 seconds
-
3 seconds
-
4 seconds
-
-
Which of the following has not been shown to affect CRT in children?
-
Age
-
Site of measurement
-
Ambient temperature
-
Gender
-
-
Which of the following physiological parameters has CRT not been shown to correlate with?
-
Superior vena cava flow
-
Systemic vascular resistance index
-
Vena cava oxygenation ≥70%
-
Stroke volume index
-
-
Concerning CRT, which of the following is true:
-
A prolonged CRT is highly sensitive for detecting serious illness in children presenting to primary or secondary care
-
A prolonged CRT always means that the child requires a fluid bolus
-
CRT is useful in estimating the degree of dehydration in a child at risk of dehydration
-
CRT is usually shorter in neonates than in children
-
-
Which of the following sites have not been described for checking CRT in children?
-
Sternum
-
Fingers
-
Toes
-
Ear lobe
-
Answers are on page 116.
Answers to the quiz
-
(1) C. (2) D. (3) B. (4) C. (5) D.
References
Footnotes
-
Search strategy The PubMed database was searched in August 2013 with the following phrase: ‘capillary refill time’ and limited to children (aged 0–18 years). Eighty-five articles were found and screened for relevance. The references and linked articles of the relevant articles were checked to ensure no other studies were missed.
-
Acknowledgements DK would like to express his gratitude to the Yorkshire and Humber Postgraduate Deanery for funding his year as a clinical leadership fellow in research.
-
Contributors DK conceived the idea for this article. All authors were involved in writing and reviewing the final manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Commissioned; externally peer reviewed.